Conditions Treated
The Center for Pediatric & Adolescent Gynecology provides comprehensive evaluation and personalized treatment for common and rare conditions affecting the female reproductive system of infants, children, adolescents and young adults. Some of the conditions we evaluate and manage are listed below.
Adolescent Health & Initial Visits
The American College of Obstetrics & Gynecology (ACOG) recommends that teenagers between ages 13 and 15 years see a gynecologist for a well adolescent visit, to discuss healthy lifestyle habits and to review preventive health care options. This visit is a great opportunity for answers and education. Generally, a pelvic exam is not necessary at this visit.
Pelvic Pain
Pelvic pain is a common complaint in both adolescents and young women. There are many etiologies of pelvic pain and non-gynecologic etiologies, such as appendicitis, must be considered when evaluating pediatric and adolescent patients. The causes of pelvic pain are generally divided according to whether the onset is acute or chronic. Dr. Amesse has over 20 years experience in evaluating these conditions and is highly skilled in their surgical and medical management. When surgery is required, Dr. Amesse often uses minimally invasive approaches with every consideration given to preserving future reproductive function.
Acute Pelvic Pain
Adolescents with acute pelvic pain need to be evaluated urgently. Some serious
conditions that need emergent management include ovarian-tubal torsion, ovarian
cysts, ectopic pregnancy and pelvic inflammatory disease.
Chronic Pelvic Pain
Chronic pelvic pain is also expediently evaluated so as to avoid long-term conditions that diminish quality of life. A particular focus of our practice is endometriosis that is often under diagnoses in this age group and for which there are both medical and surgical options. Other causes of causes of pelvic pain include pelvic adhesions, and lingering infections.
Labial Adhesions
Labial adhesions occur when the labia minora adhere together. They are most commonly seen in girls ages 3 months to 6 years. They are often asymptomatic, although urine dribbling may sometimes occur. Labial adhesions are generally managed conservatively and are often resolved by application of topical agents.
Congenital Anomalies
Abnormal structural development of the vagina, uterine cervix, uterus, and fallopian tubes can result in a wide range of anomalies. These anomalies can become apparent either in early childhood or adolescence depending on the type of abnormality. Some abnormalities include imperforate hymen and transverse vaginal septum as well as utero-vaginal agenesis and other uterine structural defects. Dr. Amesse is experienced in evaluating and managing these developmental disorders. Many conditions can be managed medically, while others will require surgical intervention.
Abnormal Menstruation
Each young woman’s menstrual period is unique. In general, normal menstruation occurs every 28 days, with a normal range between 21-35 days, and lasts for a 4-7 day duration. The amount of bleeding can vary. In general, less than 80mL of blood loss per cycle is considered within normal ranges. Adolescent menses often differ from menses in adult women in that their menstrual cycles can be irregular at the onset and as the young woman matures they become regular.
IRREGULAR AND PAINFUL PERIODS
Often the hormonal pathways that regulate menstruation are not completely established when menses begin in adolescence. This can result in irregular and occasionally painful menstruation. We have a number of treatment options available to manage irregular and painful menses in adolescents.
HEAVY MENSTRUAL BLEEDING
Heavy menstrual bleeding is common complaint in adolescents. In nearly one-half of all cases, it is hormonal in etiology. However, it can be the first sign of an underlying bleeding disorder and this will require additional testing. Not all bleeding disorders present with life-threatening hemorrhaging, as is the case with hemophilias, and many go unrecognized. Families with undetected bleeding disorders often consider excessive menstrual bleeding normal in part because their mothers, sisters, aunts and grandmothers may have experienced heavy periods. Dr. Amesse is recognized nationally as an expert in evaluating and managing these disorders.
AMENORRHEA (ABSENCE OF MENSES)
Irregular menstrual cycles are experienced by a number of adolescents and in most cases, this will self-correct over time. However, the lack of menstruation by age 15 years or amenorrhea for 3-6 months post menarche warrants gynecologic evaluation and additional studies.
Polycystic Ovary Syndrome
Polycystic Ovary Syndrome, also known as PCOS, is a common endocrine disorder that is seen in 4%-6% of adolescents and young women. Despite this, the pathophysiology, clinical features and management of PCOS have changed over time and continue to undergo changes. The disorder is associated with hormonal imbalances, particularly androgen excess. Symptoms frequently seen with PCOS include irregular periods, excess hair growth, acne, and weight gain. An ultrasound examination will often demonstrate a mildly enlarged ovary with multiple small follicles. Dr. Amesse will work with you to find the right treatment plan to manage this chronic condition.
Adrenal Abnormalities
Adrenal gland abnormalities are often overlooked as an etiology of hormone excess in adolescents and young women. Adrenal gland disorders are not as common as ovarian disorders, but some of their symptoms, such as excessive hair growth, can mimic those seen in Polycystic Ovary Syndrome. Distinguishing between these etiologies is important so that appropriate treatment plans can be initiated early. Dr. Amesse has particular expertise in detecting and treating endocrine disorders of the adrenal gland.
Care of Patients with Developmental Delays
Often patients with developmental delays will have menstrual hygiene concerns and experience heightened premenstrual syndrome (PMS) symptoms. Dr. Amesse is an acknowledged expert in assessing these conditions. He will work with both the patient and her family to develop a personalized treatment plan.
Contraception
Pregnancy prevention is often a need of teenage girls and we can discuss multiple options now available. Oral contraceptive pills and injectable hormonal contraception, such as Depo-Provera®, are commonly used. We also provide longer acting methods such as Nexplanon®. The contraceptive patch is another good method of contraception. Additionally, the intrauterine device (IUD) is now considered an excellent option for pregnancy prevention in teens.
Vulvovaginitis
Vaginitis and vulvitis, in general, refer to a broad category of inflammatory conditions involving the vagina and vulva, respectively. When inflammation involves both areas, the term vulvovaginitis is applied. Inflammation affecting the genitalia can result in redness and discharge and cause irritation, itching, and painful urination. Dermatologic conditions and underlying systemic disorders can coexist with vulvovaginitis and must be distinguished from inflammatory causes.
At puberty the female vagina and vulva undergo significant changes. Owing to these changes, the etiologies of vaginitis and vulvitis in the prepubertal child and the adolescent will often differ.
- Prepubertal Child: Vaginal discharge is a common complaint in both pre-adolescent and adolescent girls. In some cases, it is a sign that a foreign body is present or of an underlying local or systemic condition. In children, vaginitis is most often non-specific in etiology and treatment options will be individualized according to the specific needs of the patient.
- Adolescent: The vaginal mucosa (epithelium) becomes estrogenized during puberty, rendering the vagina more resistant to bacterial infections. As a consequence, there is a shift in the causal organism and the etiologies become more specific than those seen in the prepubertal child. It may also be an indication of cervicitis secondary to a sexually transmitted infection.
Sexually Transmitted Infections
Sexually transmitted infections (STI) are epidemic among adolescents. Approximately one fourth of adolescents between ages of 14 to 19 years have had a sexually transmitted infection. Early detection and treatment of STIs are crucial to preserving future reproductive function. The Center for Pediatric & Adolescent Gynecology screens for and treats a variety of sexually transmitted infections, including Chlamydia, N. gonorrhea, Herpes, Human Papilloma Virus (HPV) and Trichomonas.
Disorders of Puberty
Puberty is a major developmental milestone that marks the transition from childhood into adolescence. Complex endocrine and physiological events orchestrate the appearance of secondary sexual characteristics, growth acceleration and reproductive system changes that will culminate in the young woman becoming fertile. Abnormal pubertal development can occur at any time during the maturation process. These disorders are categorized according to whether puberty is early or delayed. Dr. Amesse is an acknowledged expert in evaluating and managing puberty disorders in young patients affected with these conditions.
EARLY OR PRECOCIOUS PUBERTY
Early or “precocious” puberty is a common disorder seen in pediatric & adolescent gynecology patients. There has been some controversy as to the appropriate age at which the child should be evaluated for signs of early puberty. Precocious puberty has been defined as puberty occurring prior to age 8 years in girls. However, recent guidelines indicate early puberty should only be considered when the signs of puberty occur before age 7 years in girls of Caucasian ancestry and 6 years, in African Americans.
DELAYED PUBERTY
Delayed puberty is usually considered when a girl fails to show signs of secondary sexual development by age 13 years, provided she in not involved in competitive, endurance sports or has a debilitating, chronic illness.
Fertility Preservation
The staff at the Palm Beach Pediatric and Adolescent Gynecology Center as in conjunction with Fertility Florida encourages the families of adolescents of all ages to consider fertility preservation options when their child is under consideration for medical or surgical treatments that may compromise their child’s future reproductive potential. We offer a number of options for fertility preservation depending on the needs of the patient.
Visit our Fertility Florida Website for more information! Click Here.
Female Services:
- Egg Vitrification: Egg vitrification is a cutting-edge technology that is used at Atlantic Reproductive Associates. It is a process where oocytes or eggs are harvested from the ovaries using a minimally invasive ultrasound-guided procedure. The retrieved eggs are transferred to a special media and kept at a very low temperature where they can be maintained indefinitely for future use. The vitrified eggs can then be fertilized at a later date, grown in vitro and then transferred to the woman’s uterus.
- Embryo Cryopreservation: This process is similar to egg vitrification, but differs in that the egg is fertilized and grown in culture and then cryopreserved. The cryopreserved embryos can then be thawed and transferred to the prepared uterus at a later date.
- Other Methods: Hormonal suppression of the ovaries has been shown to help preserve ovarian function during radiation and chemotherapy treatments, and this is an option that is available. Another option, orchiopexy, is to surgically move the ovaries out of the radiation field.
Male Services:
- Sperm Freezing: Semen samples are collected, placed in special media and cryopreserved using standard procedures. When needed, the specimen can be thawed and used to fertilize an egg either in utero or in vitro.
Ovarian cysts
Ovarian cysts are quite common in the adolescent population, but need to be treated with care and diligence. In most cases they are benign and will resolve spontaneously. However, in some cases they become quite large. A concern is that the ovary can become twisted and the blood supply will be shut off. In some cases, they will cause pain and will need to be removed. Most of the time this can be done on an outpatient basis with the patient going home on the same days. A common benign cyst is a dermoid. These cysts are solid and will not resolve on their own and will require more extensive surgery. If the cysts appear to be malignant then appropriate referrals to a gynecologic oncologist will be made.
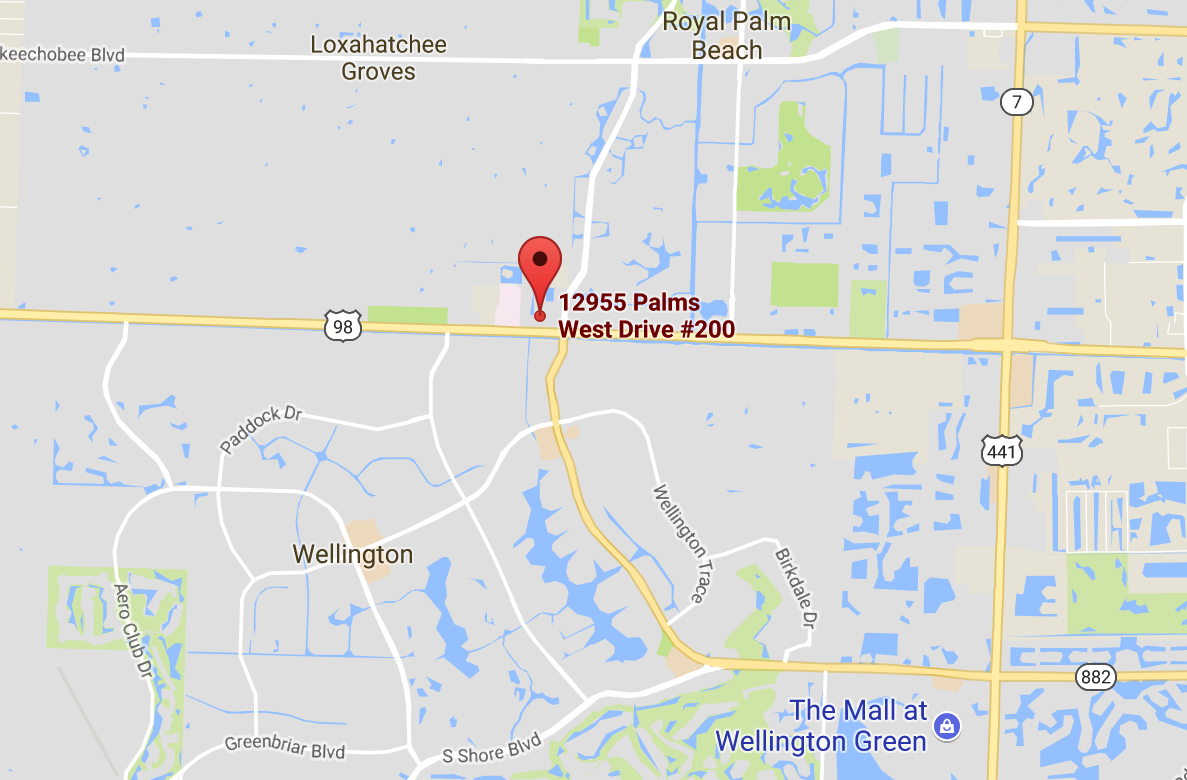
CENTER FOR PEDIATRIC & ADOLESCENT GYNECOLOGY
12955 Palms West Drive Suite 200
Loxahatchee, Florida 33470
T:561-257-0816
F:561-257-0817
Email: amesse@fertilityflorida.com